Impact of Sexual Lifestyle on Hormone-Related Health Decline Case Married Teachers
Zerf Mohammed
Physical Education Institute Laboratory OPAPS, University of Mostaganem, Mostaganem, Algeria. |
AbstractThe study aimed to evaluate the impact of accumulation hormones on health decline among some married teachers from the middle school. Founded on the background which confirmed in one hand, that any hormone, natural or synthetic, has the potential to cause unwanted side effects. While in another hand, the report of similar studies confirms that profession of teaching increased obesity, due to working conditions which do not encourage the practice of physical activity. For the purpose, our sample is consisting of 34 married teachers, their average age ≤ 26,32±3,12. They accepted to venous blood withdrawal under fasting conditions and anthropometric measurement (body weight, body height and body mass index).The only differences between them are in the method of avoiding pregnancy. The datum was performed by SPSS 19 using Levene statistic,Shapiro-Wilk, T-test independently and correlation of Pearson.
|
Licensed: |
|
Keywords: |
1. Introduction
Recognise that overweight/obesity has a multifactorial source, different genetic, metabolic, behavioural (habits and physical activity), environmental, cultural and socioeconomic factors that have contributed to its appearance. Although, similar studies confirm that the teaching profession is associated with obesity due to work conditions, which have contributed to the development of lifestyle-related illnesses (Leiva, Marchant, Ruggeri, & Saulo, 2015). Therefore, The most know that major hormonal changes occur in women with significant alterations in body weight (Wijma & Von Schou, 1992).
While the Hormones are incredibly vital chemical messengers in your body (Vincent, 2006) they surge through our bodies and cause a state of heightened awareness, usually in times of danger (Sally, 2014). It is impossible to overstate their fundamental role in the healthy functioning of the human body and in the normal progression from infancy through puberty (Nisha, 2006) whereas natural hormones are not expected, due to their short half-life (Tõnu, 2007). While physicians argue that synthetic hormones carry an additional risk to the health (Phyllis, 2006) as brain, heart, bones, muscles, and reproductive organs according to Linda (2005); Richard and Matthew (2011).
Check out the health status of our sample, which relies on birth control pills that contain synthetic versions of estrogen and progesterone (Scholastic Library Publishing, 2005). While Claudia Welch confirmed that women who had used the contraceptive pill had risks of synthetic hormone use at any stage of a woman's life. Although Jane and Melvyn (2005) confirm in one hand that pill contraceptive has strong side-effects and relatively low reliability on another it is not recommended as the main method of birth control.
While the oral contraceptive pills are the most widely prescribed medications for women.
Seen this reality, our aims in this study focused on the impact of accumulation hormones on health decline and their relationships with lipid profiles and body mass index among the married teachers in order to provide baseline information for future analytical studies.
2. Methodology
All variables were determined using commercial kits (laboratory of Dr. Bajaj Committee Zhana). All analyses were run in duplicate for the two groups. All results used in this research are derived from a medical assessment of passions.
2.1. Subjects
We studied a sample of 34 married teachers 17 who practices the traditional method (the day of ovulation) and those who takes pills, their average age 32,75±1,02 years during the academic year 2015-2016. They were selected by the intentional method because they voluntarily agreed to venous blood withdrawal under fasting conditions. All participants were healthy non-smokers not engaged in planned physical activity and not taking any medication on a regular basis. They were informed about procedures and all provided their written consent.
2.2. The Study Protocol
Our protocol was validated by the professor of physiology and nutrition the Institute Physical Education and the Sport University of Mostaganem.
- As the conditions, we are focused on:
![]() The same social status and marital lifestyle education.
The same social status and marital lifestyle education.
![]() The entire sample is married teachers with the same obligations.
The entire sample is married teachers with the same obligations.
![]() Our protocol is based on blind sample
Our protocol is based on blind sample
![]() The practice test was during medical visits by the occupational physician.
The practice test was during medical visits by the occupational physician.
![]() Our sample does not practice any sports.
All the test was done 7 days before menses.
Our sample does not practice any sports.
All the test was done 7 days before menses.
- Required tests Resources:
- Anthropometric measurements
Body mass was measured to the nearest 0.1 kg and body height to the nearest 0.5 cm using standard medical equipment in subjects wearing light indoor clothing without shoes, jackets and sweaters. Body mass index (BMI) was calculated as body mass (kg) divided by height (m) squared.
- Blood tests
- Estradiol test is a blood test.
An estradiol test is a blood test that measures the amount of estradiol in your blood. It’s also called an E2 test. Estradiol is a form of the hormone estrogen, and it’s also called “17 beta-estradiol.” The ovaries, breasts and adrenal glands make estradiol. During pregnancy, the placenta also makes estradiol. Estradiol helps with the growth and development of female sex organs, including the: uterus-fallopian tubes-vagina-breasts. Estradiol helps to control the way fat is distributed in the female body. It’s also essential for bone and joint health in females. Janelle and Steven (2015) whereas Medical Encyclopedia seat that Birth control pills can affect test Daniel, David, and Isla (2015) results based on that we agree that more estrogen return to synthetic. Borawski and Bluth (2011); Carmina, Stanczyk, and Lobo (2014) The serum estradiol level in young women with normally functioning ovaries ranges between 100 and 300 pg/ml. Togas and David (2003) around 100–150 pg/mL during the period from –10 to –5 days before menses (Jill, Karen, & Nori, 2007).
Before menopause, estradiol levels are widely variable throughout the menstrual cycle (Alina, 2015):
Mid-follicular phase: 27-123 pg/mL
Periovulatory: 96-436 pg/mL
Mid-luteal phase: 49-294 pg/mL
Postmenopausal: 0-40 pg/mL
- Progesterone test
Progesterone is a hormone that your body produces. Both men and women produce it. But it’s mainly produced in the ovaries, which means women tend to have more of it.
2.3. Normal Test Results
In general, normal serum progesterone test results fall within the following ranges:
Serum progesterone level of 10 ng/mL (31.8 mmol/l) to 20 ng/mL or greater 1 week before menses (Richa, 2014). While Cynthia C Chernecky and Barbara J Berger seat that pill contraceptive contains 0,1-0,3 ng/mL (Cynthia & Barbara, 2013). Based on that we agree that a more Progesterone return to synthetic
2.4. Statistical Analyses
Baseline characteristics of the participants are presented in Table 1. According to Shapiro-Wilk and Levene's test person correlation, our total sample accepts the normally distributed, homogeneous and total positive linear correlation between the parameters chosen to study in the exception of Progesterone which is strongly negative. Whereas Estrogen pg./ml is over the norms seated Togas Tulandi and David Redwine confirmed by John (2012) and Donna (2016) in opposite of Progesterone which is in norms seated by Marc and Leon (2012) and Richa (2014) whereas BMI of our total sample is overweight according to the standards of World Health Organization (2010).
| variables | means ± SD |
Levene's test |
Shapiro-Wilk |
Correlation |
|||
F |
Sig. |
W |
Sig. |
R |
Sig. |
||
| AGE | 26.32±3.12 |
0.10 |
0.75 |
0.95 |
0.23 |
0.91 |
00 |
| Weight | 66.10±7.86 |
0.40 |
0.53 |
0.94 |
0.11 |
0.53 |
0.02 |
| Height | 1.62±0.04 |
0.58 |
0.59 |
0.96 |
0.19 |
0.99 |
00 |
| BMI | 29.36±4.03 |
2.41 |
0.13 |
0.95 |
0.12 |
0.61 |
0.01 |
| Estrogen pg./ml | 167±0.03 |
2.08 |
0.81 |
0.97 |
0.45 |
0.96 |
00 |
| Progesterone ng/mL | 15.76±3.39 |
0.79 |
0.38 |
0.95 |
0.12 |
-0.51 |
0.04 |
Source: Baseline characteristics of all subjects (Anthropometric Vs Blood tests used in present study). |
3. Results
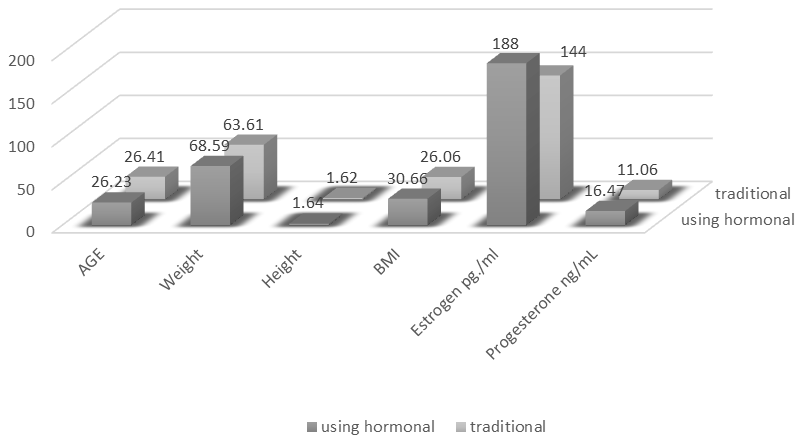
Based on the data tests and the data analysis procedures used in this study consisted of the computation of the means, standard deviations and the independent T-test as Descriptive statistics. With a Significance level was set at 0.05. All the compare T are not significant in AGE, Weight and Height in the opposite of BMI, Estrogen and Progesterone in the benefit of a traditional method based on the normative medical seat in Required Tests Resources.
| variables | sample | N |
means ± SD |
T |
Sig. |
| AGE | using hormonal | 17 |
26.23 ±3.01 |
-0.162 |
0.87 |
| traditional | 17 |
26.41±3.29 |
|||
| Weight | using hormonal | 17 |
68.59±8.17 |
1.92 |
0.08 |
| traditional | 17 |
63.61±6.89 |
|||
| Height | using hormonal | 17 |
1.64±0.04 |
0.04 |
0.99 |
| traditional | 17 |
1.62±0.07 |
|||
| BMI | using hormonal | 17 |
30.66±4.53 |
1.99 |
0.00 |
| traditional | 17 |
26.06±3.09 |
|||
| Estrogen pg./ml | using hormonal | 17 |
188±0.02 |
3.39 |
0.00 |
| traditional | 17 |
144±0.03 |
|||
| Progesterone ng/mL | using hormonal | 17 |
16.47±2.83 |
3.34 |
0.00 |
| traditional | 17 |
11.06±3.09 |
Source: Baseline characteristics of sample (Anthropometric Vs Blood tests used in present study) based on Sexual Lifestyle method. |
4. Discussion
Through the Table 2 and Figure 1 all the comparisons are in the benefit of traditional method group record in BMI, where our traditional group is Overweight in opposite the sample using hormonal which is Obese. Whereas these results line with normative WHO that Overweight defined as 25≤ BMI < 30; obesity defined as BMI ≥30 (Robert, Douglas, & Douglas, 2011). Although as sexual lifestyle hormone-related health decline, we agree that BMI ≥30 is a risk factor for high blood lipids, hypertension, diabetes and obesity (Wener & Sharon, 2016). Furthermore, the data showed that BMI increased in both active and inactive (Wener & Sharon, 2015) the case of our total married teachers, where this leads us to confirms on one hand that Any hormone, natural or synthetic, has potential to cause unwanted side effects. While the literature shows that side effects hormonal methods Steroid hormones have dominated during the past 40 years, with more than 200 million women which risk obesity (Bloomsbury Publishing, 2005) well on other hand, we approve the results of Taiwanese study which reported that 15 minutes of daily physical activity reduced all-cause mortality (David, 2013). While as a lifestyle, we refer to Potter and Paschke (2016) which Recommended the aerobic exercise at 3 to 5 times per week for approximately 30 minutes (Patricia, Anne, & Patricia, 2016). Cross, this evidence, that hormonal contraceptives increase weight gain and high-density lipoprotein cholesterol concentrations (Roberts, Paul, & Margaret, 2013); (Teri & Marylou, 2015). Our results are in conformity with provided by Kerri and Frances (2016) and Mira (2015) the case of weight gain (Kerri & Frances, 2016); (Mira, 2015) due to the technique contraceptive and lifestyle choice by the woman and her partner according to Zerf (2016). To conclude we agree, that hormone-related health decline is a complex metabolic disorder, with numerous genetic and environmental factors interacting and contributing to the pathophysiologic features according to Amanda, Steven and Ryan (2016); Zerf (2015); Page and Holmes (2009). However, these results are in conformity with the indicated which agree that profession of teaching increased obesity due to lack of physical activity in our case, we approve that married teachers using hormonal contraceptives risks fatness confirmed in values of BMI and overweight in the opposite of teachers using the traditional method due to levels Estrogen and Progesterone. While The Women's Health Initiative (WHI) found that women taking estrogen and progestin were at increased risk of myocardial infarction, stroke, venous thromboembolism, and breast cancer as compared with women taking placebo according to Jennifer Hays, et al.
5. Conclusions
Based on the standards specified by our physicians quoted in testing resources data, our results line with the diagnosis of Dagny (2007) the same hormones that birth control pills (and other hormone-containing birth control methods) regulate to prevent pregnancy can affect the way your body feels and functions (Dagny, 2007). Whereas our account T-test confirms that Too much of synthetic hormone can cause bloating, depression, fatigue, increased hair growth on the body, and increased weight gain according to Philip (2012) thing confirms by Swartz and Wright (2015) that the Doctors are reading and hearing that estrogen and progesterone cause heart disease (Swartz & Wright, 2015). Where women with the following health problems should avoid birth control pills (Judith, 2010) due to a Hormonal imbalance which is often incriminated in women taking contraceptive pills. Arveen and Michael (2012) From proofs, our results line with discernment described by Philip Maffetone, that medications have potential side effects that can impact our health, muscle strength, metabolism, and other systems of the body that promote health and fitness (Philip, 2015).References
Alina, G. S. (2015). Estradiol. Retrieved from http://emedicine.medscape.com/article/2089003-overview .
Arveen, K., & Michael, L. C. (2012). Kumar and clark's clinical medicine. USA: Elsevier Health Sciences.
Bloomsbury Publishing. (2005). Black's medical dictionary. London: A. & C. Black.
Borawski, D., & Bluth, M. H. (2011). Reproductive function and pregnancy. In: McPherson RA, Pincus MR, eds. Henry's Clinical Diagnosis and Management by Laboratory Methods (2nd ed.). Philadelphia: Elsevier Saunders, PA.
Carmina, E., Stanczyk, F. Z., & Lobo, R. A. (2014). Laboratory assessment. In: Strauss JF, Barbieri RL, eds. Yen and Jaffe's Reproductive Endocrinology (7th ed.). Philadelphia: Elsevier Saunders, PA.
Cynthia, C. C., & Barbara, J. B. (2013). Laboratory tests and diagnostic procedures. St. Louis, Mo: Elsevier Health Sciences.
Dagny, S. B. (2007). Runner's world complete book of women's running: The best advice to get started, stay motivated, lose weight, run injury-free, be safe, and train for any distance. Emmaus, PA: Holtzbrinck Publishers.
Daniel, N. S., David, Z., & Isla, O. (2015). In estradiol blood test. Retrieved from https://medlineplus.gov/ency/article/003711.htm.
David, H. (2013). Health promotion and aging: Practical applications for health professionals. New York: Springer Publishing Company.
Donna, L. (2016). Clinical chemistry: Fundamentals and laboratory techniques (1st ed.). USA: Saunders.
Jane, C., & Melvyn, D. (2005). Anatomy and physiology for midwives. New York: Churchill Livingstone/Elsevier.
Janelle, M., & Steven, K. (2015). In health line media. Retrieved from http://www.healthline.com/health/estradiol-test#ReadThisNext7 .
Jill, B. B., Karen, J. B., & Nori, G. (2007). Sex differences in the brain: From genes to behavior. UK: Oxford University Press.
John, P. (2012). Hypothalamic peptide hormones and pituitary regulation. UK: Springer Shop.
Judith, R. (2010). The disabled woman's guide to pregnancy and birth. UK: ReadHowYouWant.com.
Kerri, D. S., & Frances, E. L. (2016). Women’s gynecologic health (3rd ed.). USA: Jones & Bartlett Learning.
Leiva, V., Marchant, C., Ruggeri, F., & Saulo, H. (2015). A criterion for environmental assessment using Birnbaum–Saunders attribute control charts. Environmetrics, 26(7), 463-476. Available at: https://doi.org/10.1002/env.2349.
Linda, W. (2005). Essential anatomy and physiology in maternity care. USA: Elsevier Health Sciences.
Marc, A. F., & Leon, S. (2012). Clinical gynecologic endocrinology and infertility. USA: Lippincott Williams & Wilkins.
Mira, H.-W. (2015). Medicines for women. UK: Springer Shop.
Nisha, J. (2006). Surviving the teenage hormone takeover: A guide for moms. USA: W Publishing Group.
Page, R. D., & Holmes, E. C. (2009). Molecular evolution: A phylogenetic approach: John Wiley & Sons.
Patricia, A. P., Anne, G. P., & Patricia, S. (2016). Fundamentals of nursing. USA: Mosby.
Philip, M. (2012). The big book of health and fitness: A practical guide to diet, exercise, healthy aging, illness prevention and sexual well-being. New York: Skyhorse Publishing.
Philip, M. (2015). The endurance handbook: How to achieve athletic potential. USA: Stay Healthy. Skyhorse Puplising.
Phyllis, A. B. (2006). Prescription for nutritional healing. UK: Penguin.com.
Potter, K., & Paschke, J. L. (2016). Large-scale patterns of insect and disease activity in the conterminous United States and Alaska from the national insect and disease survey, 2014. In: Potter, Kevin M.; Conkling, Barbara L., eds. 2016. Forest health monitoring: National Status, Trends, and Analysis 2015. Gen. Tech. Rep. SRS-213. Asheville, NC: US Department of Agriculture, Forest Service, Southern Research Station, 213, 21-40.
Richa, S. (2014). Bedside obstetrics & gynecology (2nd ed.). New Delhi: Jaypee Brothers Medical Publishers (P) Ltd.
Richard, A. M., & Matthew, R. P. (2011). Henry's clinical diagnosis and management by laboratory methods. US: Elsevier Health Sciences.
Robert, O. B., Douglas, L. M., & Douglas, P. Z. (2011). Braunwald's heart disease: A textbook of cardiovascular medicine. UK: Elsevier Health Sciences.
Roberts, D. F., Paul, S. M., & Margaret, B. (2013). Mayo clinic internal medicine board review. UK: Oxford University Press.
Sally, T. (2014). Finding the river: The energy self-help manual for surviving life's challenges. USA: Dragon Rising Publishing.
Scholastic Library Publishing. (2005). Encyclopedia Americana: Heart to India. Scholastic Library Pub, Danbury Conn.
Swartz, J. M. M. D., & Wright, M. A. Y. L. (2015). The wisdom of bioidentical hormones in menopause, perimenopause, and premenopause: How to balance estrogen, progesterone, testosterone, growth hormone; heal insulin, adrenals, thyroid; lose belly fat. USA: Lulu.com.
Teri, M. W., & Marylou, V. R. (2015). Pharmacotherapeutics for advanced practice nurse prescribers. US: F.A. Davis.
Togas, T., & David, R. (2003). Endometriosis: Advances and controversies. USA: CRC Press.
Tõnu, P. (2007). Principles of food toxicology. USA: CRC Press.
Vincent, I. (2006). Degenerative diseases of ageing: Causes and preventions. UK: De-Ichekus (UK) Co. Ltd.
Wener, W. K. H., & Sharon, A. H. (2015). Principles and labs for fitness and wellness. USA: CengageBrain.com.
Wener, W. K. H., & Sharon, A. H. (2016). Lifetime physical fitness and wellness: A personalized program. USA: CengageBrain.com.
Wijma, K., & Von Schou, B. (1992). Reproductive life: Advances in research in psychosomatic obstetrics and gynaecology. UK: CRC Press.
World Health Organization. (2010). World health statistics: World Health Organization, FR.
Zerf, M. (2015). Impact of preventing pregnancy methods and their relationships with the level of growth fitness body health housewife case women newlyweds. American Journal of Sports Science and Medicine, 3(5), 90-95.
Zerf, M. (2016). Which causal relationship established the effect of the control technique contraceptives on weight gain case housewives newlyweds. International Journal of Humanities and Social Sciences, 7(1), 47-58.